



A plethysmograph is a device used to measure an alteration in volume in response to a manoeuvre or change in circumstance. It is unable to measure absolute volume or determine the reason for the volume change. Regarding the leg, it can measure the rate of volume reduction in response to leg elevation as well as the rate of volume increase in response to leg dependency. From these manoeuvres, conclusions may be drawn regarding venous drainage and venous reflux, respectively. Current research is focusing on validation to interpret the meaning of the volume changes observed.
CLAUDE FRANCESCHI Plethysmography measures a volume variation. Three methods are available, currently. Photo-plethysmography (PPG) measures the superficial blood volume just below the sensor (infrared signal). Strain gauge plethysmography (SGP) measures the circumference variation according to the gauge length variation (piezo-electric signal). This is usually the maximum calf diameter. Air-plethysmography (APG) measures the segmental volume variation according to the pressure variation inside a cuff usually around the calf (air pressure signal). Historically water-plethysmography was used, but the apparatus was cumbersome and fixed preventing elevation/dependency manoeuvres. Furthermore, there were major problems with leakage.
According to the pressure/volume relationship, the volume variations depend mainly on the emptying and filling within veins which are a result of the trans-mural pressure (TMP). This is the difference between the pressures inside, intravenous pressure (IVP), and outside, external venous pressure (EVP), the container. The compliance of the content is also important (compliance or change in volume, dV= [IVP-EVP]). Absolute TMP is not measured, only its variation.
The compliance and bulk modulus of the container are just as important as the IVP in interpreting the results of plethysmography. For example, the veins and surrounding tissues are often impaired by the fibrosis associated with lipodermatosclerosis, particularly in the context of current or previous ulcers. Interestingly, a non-invasive method of measuring IVP can be determined using a hand-held Doppler transducer over the GSV at the ankle, provided the surrounding tissues are compressible. This is similar to the principle of measuring the ankle-brachial pressure index (ABPI) in arterial insufficiency. This avoids the need for direct IVP measurements using a venous catheter. The elevation or graduated venous pole test is an alternative.
Choice of plethysmographic method remains controversial. Each has published advantages and disadvantages. Interpretation of the results in line with the provocation manoeuvres is key to providing useful information in superficial, deep and perforating veins, before and after treatment.
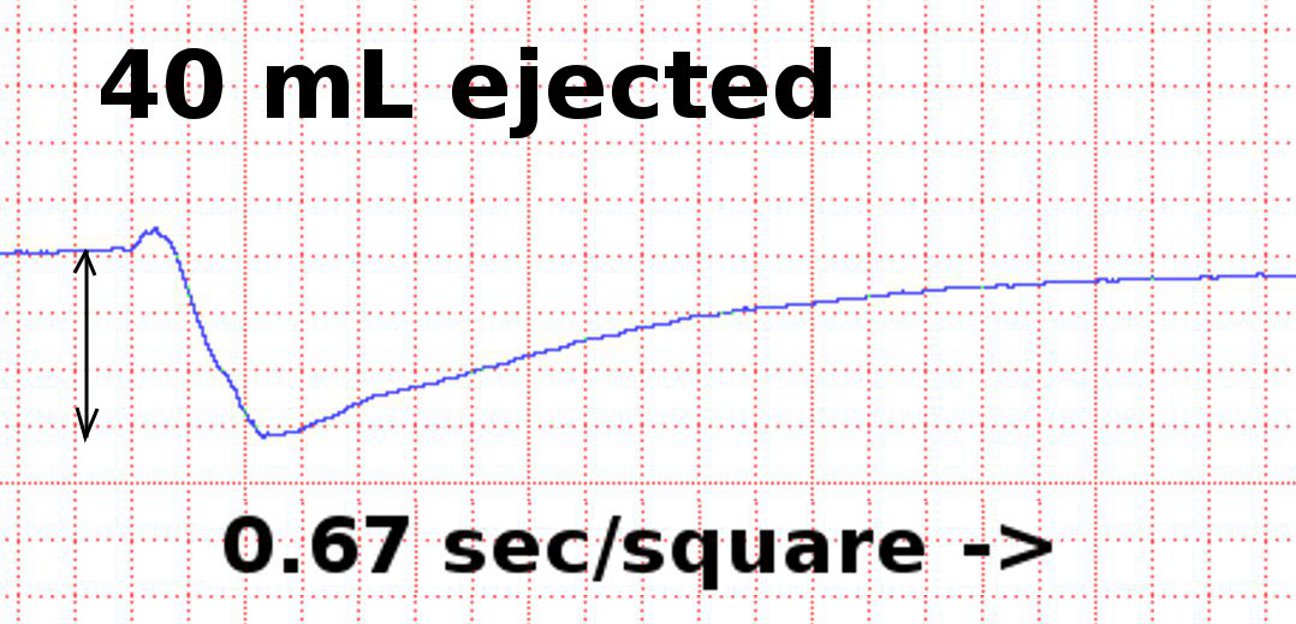
Air-plethysmography tracing (volume vs time) demonstrating the decrease in calf volume with an ankle dorsiflexion (Wunstorf manoeuvre).