



The non-invasive evaluation of an iliac vein stenosis remains a significant challenge. Furthermore, it is unclear which geometric configuration is the most important in causing resistance to flow. The minimum diameter has been proposed as a better index of resistance in contrast to a cross-sectional area reduction. This can be likened to a garden hose pipe where a moderate constriction of the outlet causes resistance with faster velocities allowing a greater distance of water coverage. Interestingly, this takes place without a reduction in cross-sectional area. Duplex ultrasound has potential in the non-invasive evaluation of an iliac stenosis, but imaging veins deep within the pelvis is often very difficult. Three ultrasound parameters have been identified which may help in the assessment of a significant stenosis:
STEPHEN F DAUGHERTY We measure the minor diameter of the vein at the stenosis and compare this to the “normal” diameter of the vein below the lesion. Most clinically significant lesions are those with a >75% diameter stenosis. However, the variable geometry of the vein affects the sensitivity and specificity of the diameter measurement to predict hemodynamically significant compression. Reversal of flow in the internal iliac vein at rest or after treadmill exercise (7 minutes, 10% gradient, 4.3 km/hr) is 100% specific for a hemodynamic and clinically significant stenosis in our experience, but the sensitivity is disappointing. A peak venous velocity (PVV) over 40 cm/sec or a PVV ratio (PVVR) over 2.5 usually suggests hemodynamic significance, but sensitivity remains a problem for these parameters. The vast majority of patients with clinically significant iliac vein compression meet one or more of the listed criteria, but many do not meet all of the criteria.
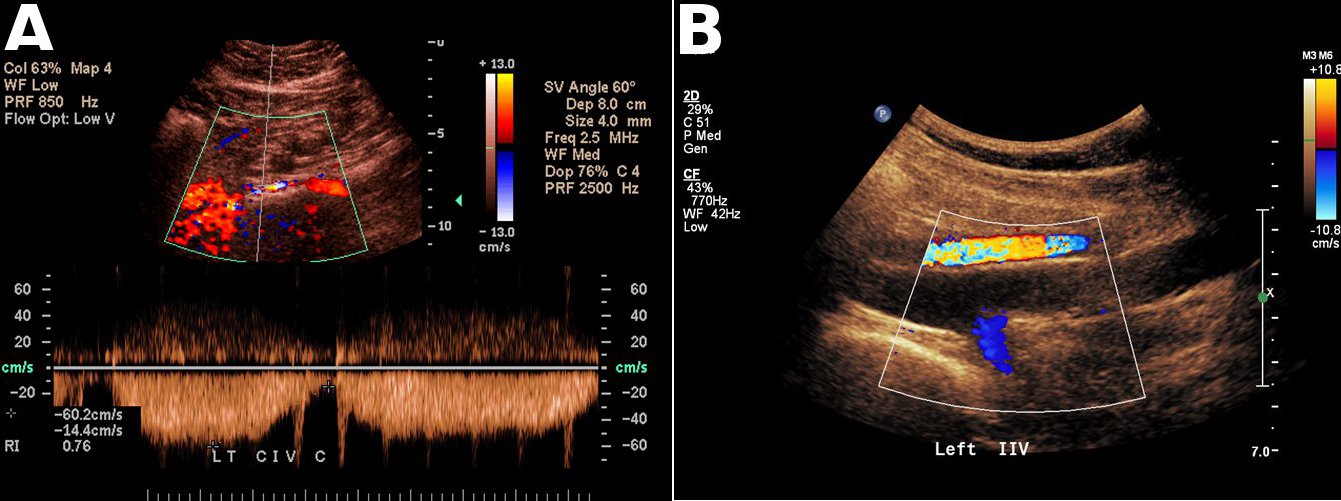
A) Elevated PVV across a high grade compression of the left common iliac vein
B) Reversal of flow in the left internal iliac vein (blue)