



A deep vein thrombosis (DVT) in the leg may cause several pathological lesions. These include obstruction, stenosis and scarring of the vein wall. Whilst imaging methods may detect the main lesions, it is likely that the DVT process affects all the leg veins, resulting in a more stiff system which is less capable of facilitating venous return to the heart. Compression duplex ultrasound and contrast venography are able to identify the obvious lesions. Some of the appearances of obstruction are illustrated below.
PETER SCHNATTERBECK The radiological appearances of veins following a DVT have an infinite number of variations. The left leg of a patient after several episodes of DVT is presented to illustrate the adaptation of the venous system in response to the new haemodynamic environment of obstruction and scarring. The images in this patient have been obtained following direct deep venous puncture and placement of a sheath through which contrast was administered. Imaging of the veins was obtained using a cone-beam CT technique.
Occasionally natural bypasses are able to accommodate the drainage of blood from the leg. If this is inadequate and the patient has continuing symptoms of venous claudication, pain, leg swelling or ulceration, then venous stenting and/or a surgical bypass may be required. The possibilities in the example provided include stenting of the iliac vein, a surgical Palma bypass or a popliteal to femoral vein bypass utilising saphenous vein (May-Husni procedure).

A) Diffuse iliac vein stenosis or Rokitansky stenosis (arrows) with cross-pelvic drainage collaterals. This is a natural left-to-right Palma bypass.
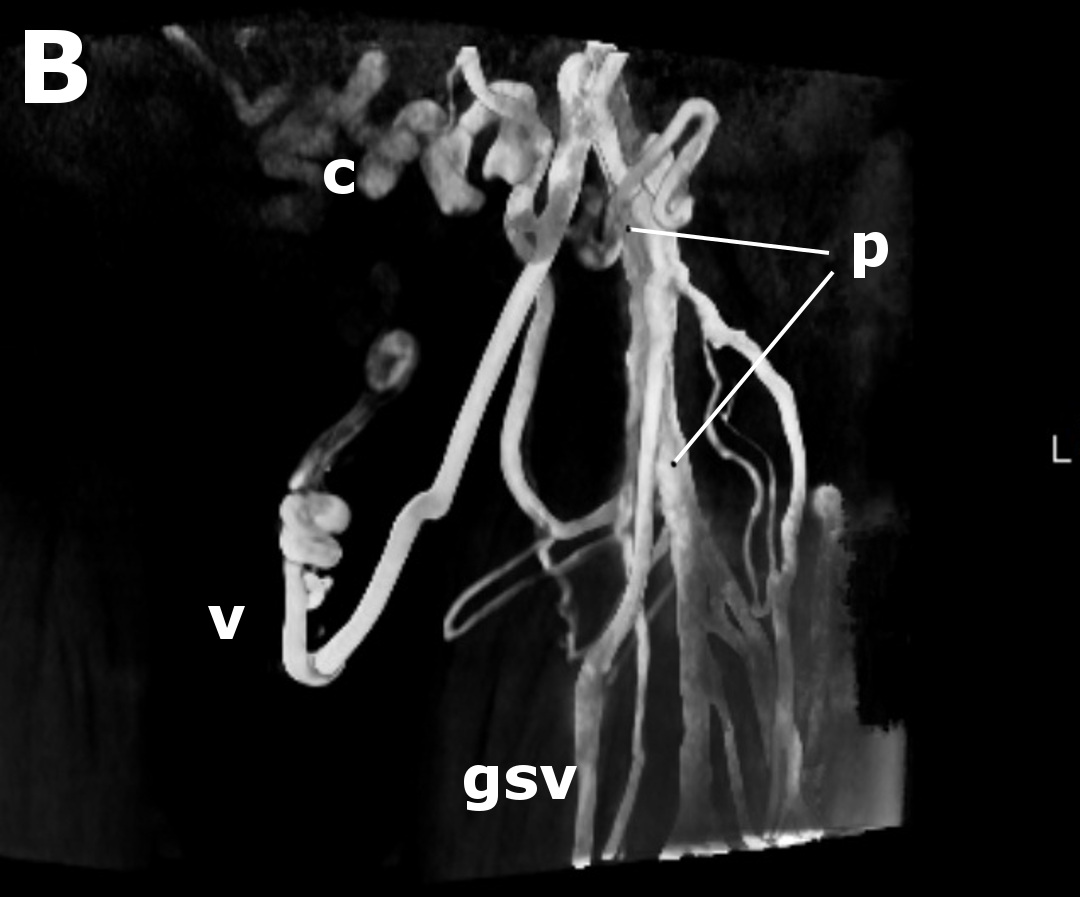
B) Upper thigh venogram of a femoral vein occlusion. Limb drainage is via the profunda femoris vein (p) and the great saphenous vein (gsv). Note the suprapubic collaterals (c) and vulval (v) drainage pathways forming a natural Palma bypass.
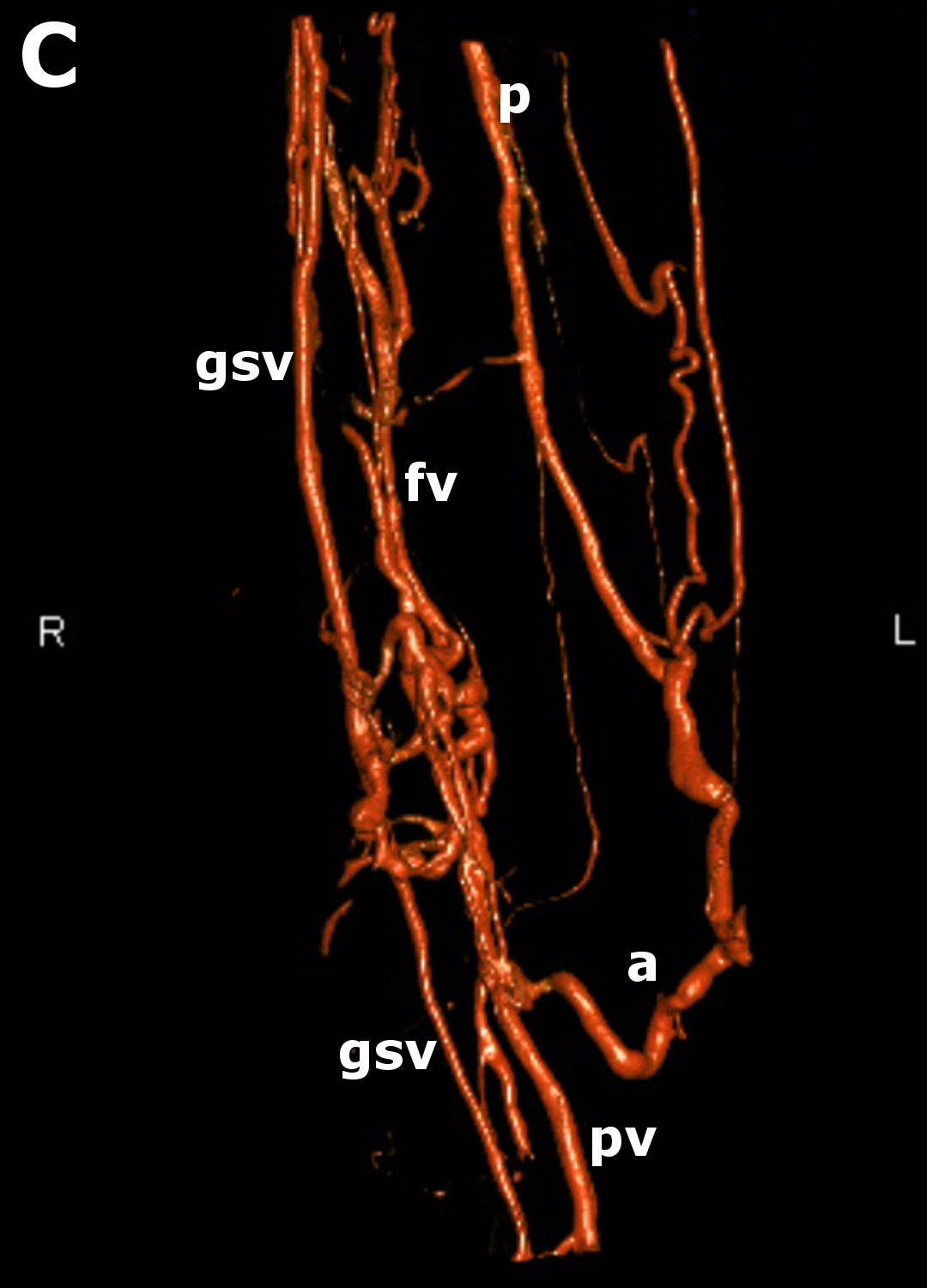
C) Lower thigh venogram of a femoral vein (fv) obstruction demonstrating poor recannalisation and peri-venous collateralisation (fv). The popliteal vein (pv) now drains into the profunda femoris vein (p) from a collateral (a). This process is termed axialisation of the profunda femoris vein. The great saphenous vein (gsv) also drains the leg. It is dilated in its upper part to accommodate the increase in drainage volume from the popliteal vein (pv). This is a natural May-Husni bypass.