



Perforating veins are those which connect the deep veins to the superficial veins. To achieve this they pass through the deep fascia of the calf. Although the sapheno-popliteal junction is a perforating vein, it is not discussed in this section. Anatomical dissections from leg amputations in patients free of venous disease reveal that the perforating calf veins are often paired and have valves preventing outward flow into superficial veins. Therefore, valve incompetence in anatomical and haemodynamic terms is outward flow during calf contraction or compression. If the diameter of the perforating vein is large this may result in skin changes or ulceration and this may be termed clinical incompetence. Interestingly, bi-directional flow has been observed in healthy legs and it is a matter of debate as to whether this is normal or represents early venous insufficiency.
Calf perforating veins are frequently the lower pole of a re-circulation circuit. These are termed re-entry perforating veins because they facilitate the re-entry of refluxive saphenous blood into deep veins. These may enlarge gradually from re-circulatory volume overload and eventually cause valve failure from dilatation of the valve ring. At this stage calf muscle contraction causes outward flow which may result in skin changes. Subfascial endoscopic perforator surgery (SEPS) is a technique originally invented by Hauer from Germany which interrupts perforating veins. This was developed and improved by Professor Nelzén as part of a group and has been shown in trials to deliver a significant clinical benefit.
OLLE NELZÉN The exact role of incompetent perforating veins are unknown. Currently there is no high-level evidence to make firm recommendations. We know that incompetent calf perforating veins are commonly associated with severe chronic venous insufficiency with skin changes, including venous ulceration. In contrast to earlier beliefs, incompetent perforating veins are intimately associated with superficial venous incompetence rather than deep venous failure. Sometimes the observed incompetence may just provide an antegrade channel for the re-entry of refluxive blood. However, two randomized controlled trials have demonstrated that only 20-30% of patients (legs) with venous insufficiency were normalized as a result of superficial surgery alone. This confirms the importance of incompetent calf perforating veins in venous disease.
In patients with venous ulceration the best available results regarding ulcer healing and recurrence were reported using a combined approach. This involves a procedure on superficial veins combined with perforating vein surgery using SEPS. The technique of SEPS is unique and novel because it provides a way of interrupting a perforating vein beneath an open ulcer. In particular, it avoids making skin incisions near an ulcer with the risk of infection and healing problems. Radiofrequency ablation techniques, laser and foam sclerotherapy are alternative approaches but these have rather high one year recurrence rates. Currently, perforating vein interruption using SEPS is the most robust solution to perforating vein incompetence.
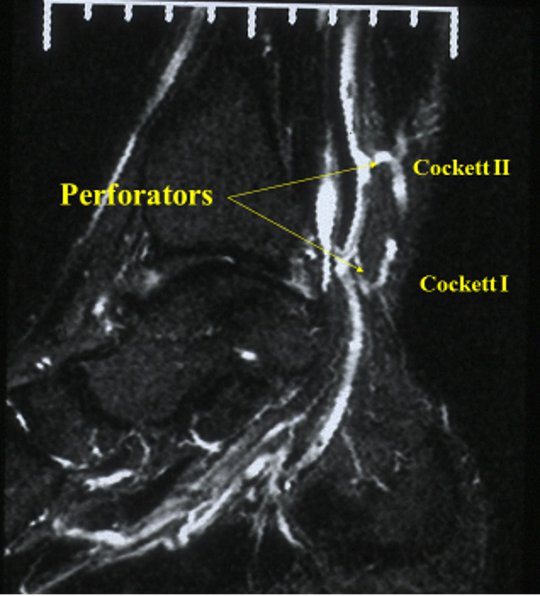 Magnetic resonance venogram (MRV) demonstrating enlarged perforating veins
Magnetic resonance venogram (MRV) demonstrating enlarged perforating veins