



Deep vein thrombosis (DVT) is a serious and relatively common thrombo-embolic event. Many remain undetected and a pulmonary embolism may be the first presentation of a silent DVT. Other mechanisms of resolution include spontaneous lysis, clot retraction, and organisation with partial recanalisation. Research into the mechanisms of lysis may unravel why some thrombi resolve spontaneously and others lead to fibrosis.
ARIE MARKEL After an episode of DVT a dynamic situation of both thrombolysis and thrombus extension occurs. The predominant activity may determine the eventual fate of the thrombus. Recanalisation is the process where an occluding thrombus undergoes changes in size, shape, and structure with eventual reestablishment of the venous lumen. This can occur after a few days with complete restoration of the normal vein architecture and luminal size. After several weeks complete resolution is less likely. The thrombus becomes organised with a connective tissue infrastructure. Recanalisation is often incomplete with the formation of endothelial lined channels within a mass of fibrosis. The mechanism of recanalisation therefore involves 2 separate processes: thrombolysis in the early stages and the formation of connective tissue channels in the later stages.
We previously demonstrated that recanalisation may occur early after an episode of DVT. After 3 years recanalisation is present in 100% of cases. This has important therapeutic implications because most chronic thrombotic occlusions can eventually be negotiated with a guide wire. However, complete recanalisation with normalization of flow can be a long protracted process. In our series, after 3 years, 50% of the legs had partial obstruction from post-thrombotic scarring.
It has been shown that early recanalisation is inversely related to levels of activated coagulation and fibrinolytic inhibition on presentation. Early recanalisation is important in preserving valve integrity and function. Obstruction is the pathology at the start with reflux predominating in the later stages of the post-thrombotic syndrome.
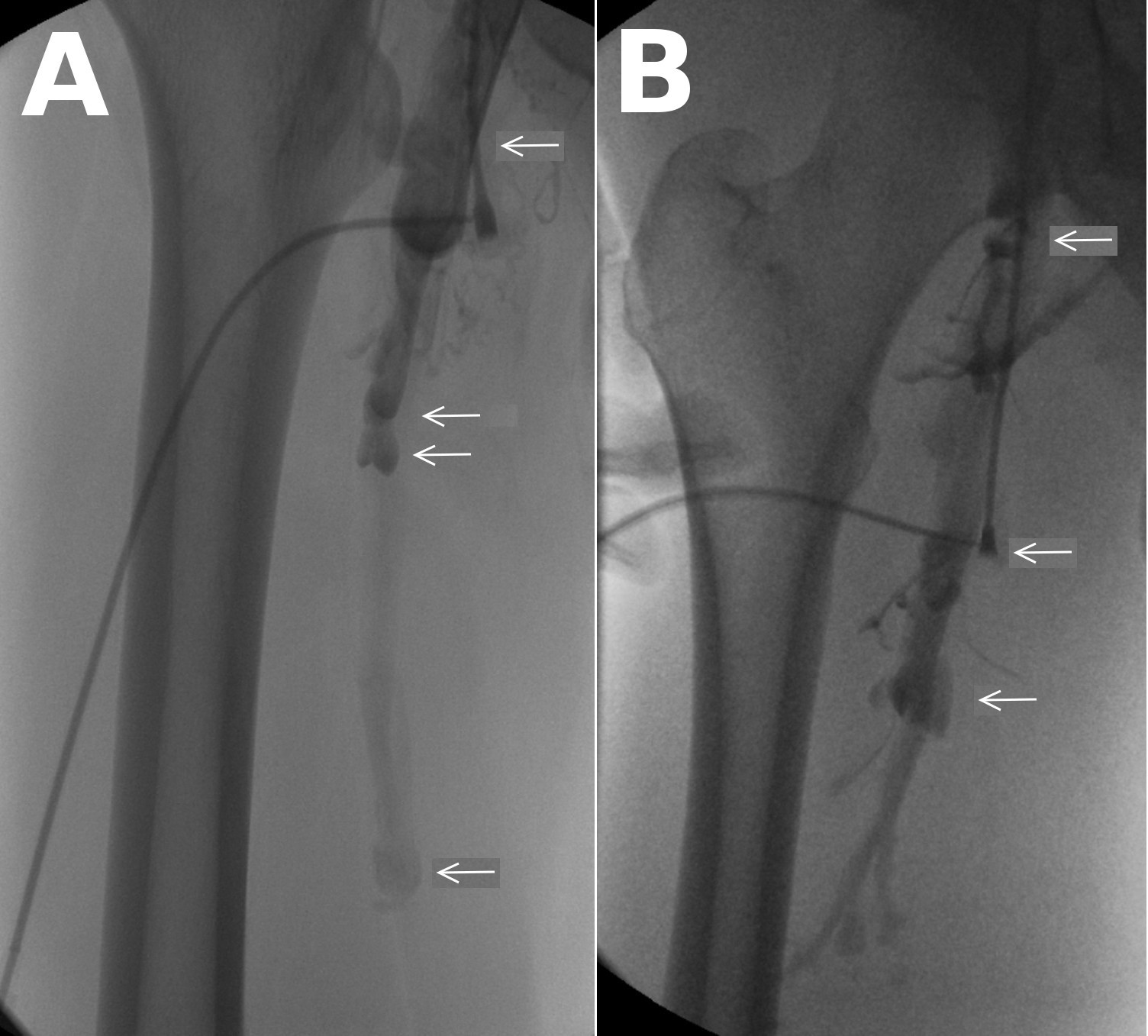
Descending venograms in 2 different patients with venous ulcers provoked using a Valsalva manoeuvre and a dependency tilt. The incompetent valve stations are marked with arrows. Retrograde flow (reflux) is seen down the superficial femoral vein (A) and the deep femoral vein (B).