



Ultrasound guided foam sclerotherapy (UGFS) is an established technique which uses ultrasound to map the direction of foam and gauge the amount required for venous closure. Contrast guided foam sclerotherapy (CGFS) is used for similar indications. However, the images provide greater detail on the behaviour of the injected foam. The amount of foam and the speed at which it escapes into deep veins can be seen with greater clarity.
LOUAY ALTARAZI In Damascus, Syria we perform contrast foam sclerotherapy in some patients to guide us how much foam to use and when we are concerned that more than a trickle of foam may enter deep veins. This may occur in patients with thigh perforating veins. The technique can be used also in complex patterns of recurrent varicose veins in the groin as well as in research to determine the effect of temporary balloon occlusion of the sapheno-femoral junction.
With balloon occlusion we can treat the GSV trunk and all its incompetent tributaries with a single injection. This technique discourages foam from entering the deep veins whilst facilitating travel into incompetent tributaries. The addition of contrast using CGFS provides us with visual feedback.
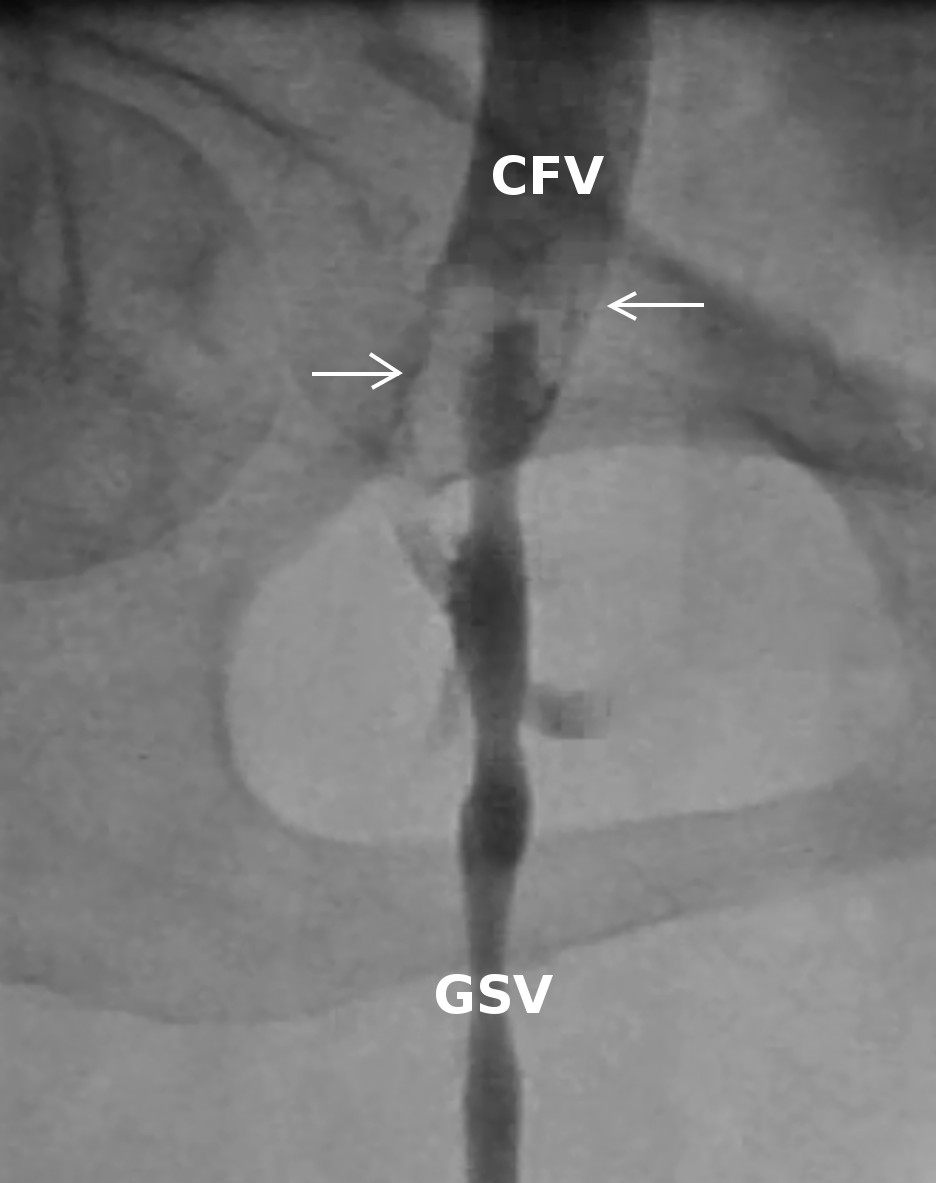
Contrast and foam has been injected into the lower great saphenous vein (GSV). Note 2 large bubbles of gas (arrows) within the common femoral vein (CFV).
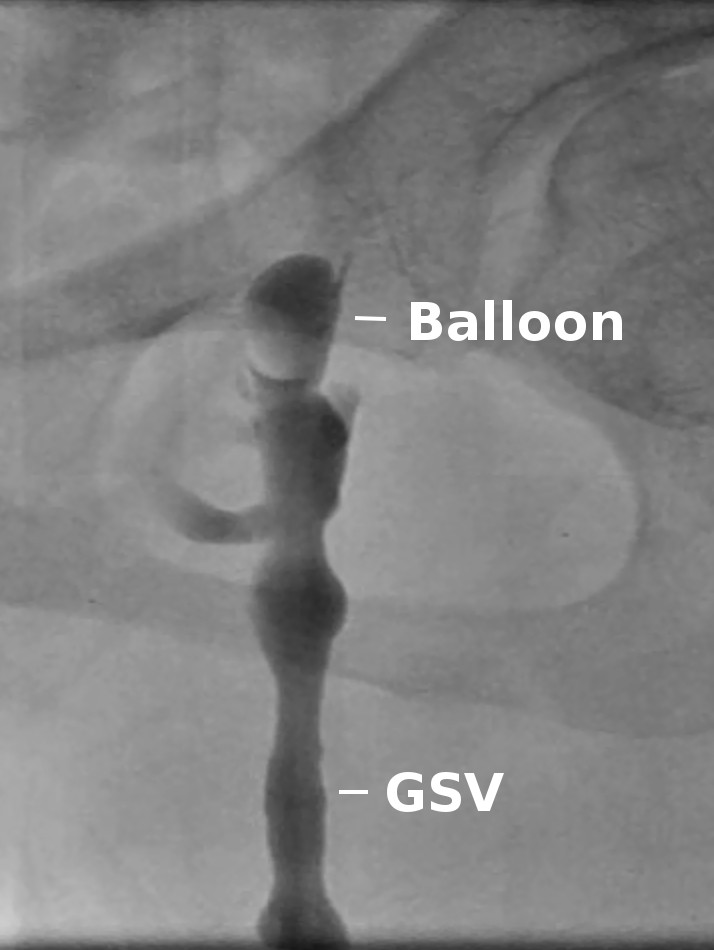
The termination of the GSV is occluded by a balloon preventing escape of foam into the CFV. Deflation of the balloon does not cause a bolus escape of foam into the CFV as assumed previously.
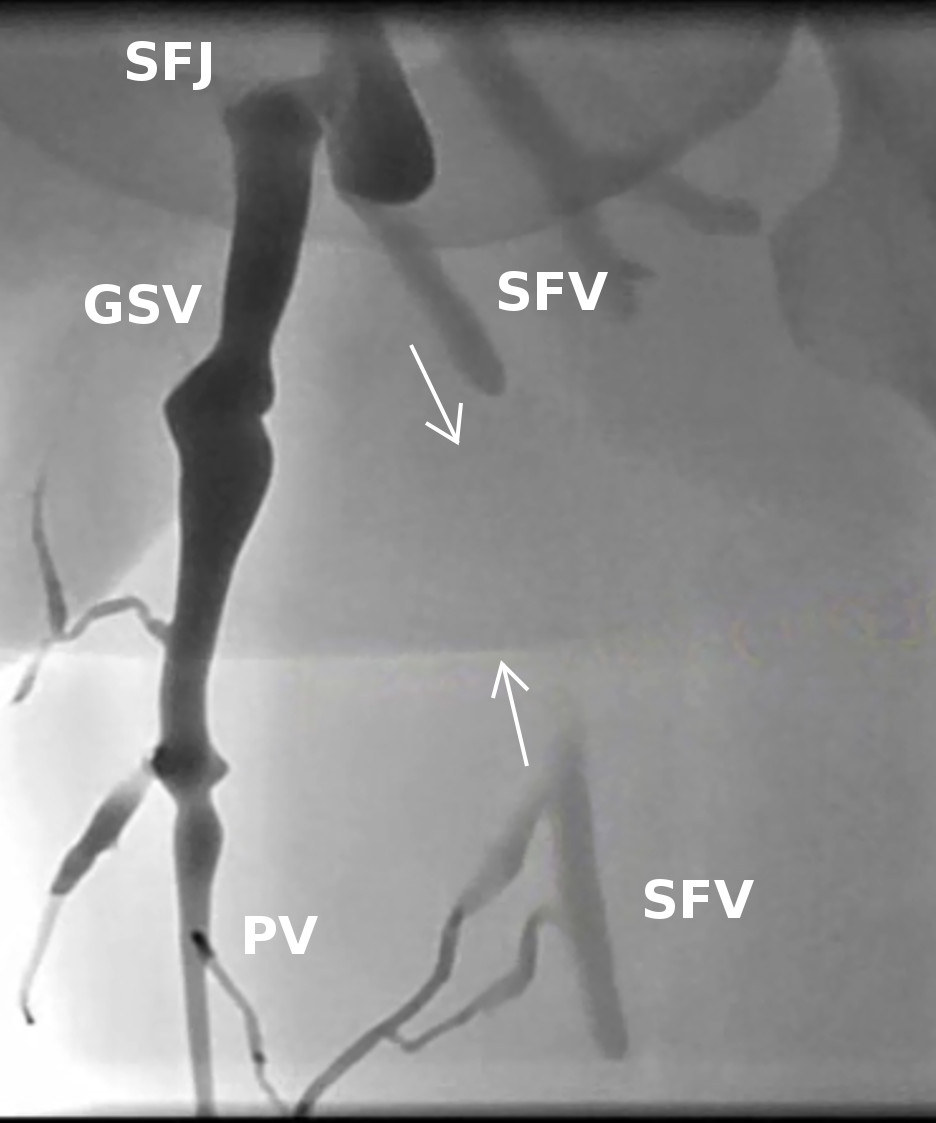
Contrast has been injected into the lower great saphenous vein. The superficial femoral vein (SVF) fills via a perforating vein (PV) and retrograde via the sapheno-femoral junction (SFJ) and common femoral vein (arrows). Balloon occlusion at the distal GSV during foam sclerotherapy prevented retrograde SFV filling, thus limiting its exposure to the sclerosant.