



The use of glue in the ablation of refluxing saphenous trunks is gaining popularity. The main advantage is that tumescence is not required. This is of benefit to the patient because the perivenous injection of fluid is uncomfortable and the procedure time is shortened. Bilateral treatments are facilitated. In common with all endovenous treatments, patient selection and operative technique are arguably more important than the device used to destroy the vein. The group from Hong Kong have extensive experience in the use of glue.
YIU-CHE CHAN These are day surgery procedures performed under local anaesthesia using ultrasound guidance. First, the great saphenous vein (GSV) is located with ultrasound and punctured percutaneously using a micro-puncture set. Then a 0.035 guide wire is passed to the sapheno-femoral junction (SFJ) and exchanged for a propriety 5 Fr long sheath. The cyanoacrylate adhesive is prepared and attached to the adhesive delivery catheter. The patient is then put in the Trendelenburg position to empty the veins. The tip of the cyanoacrylate delivery catheter is advanced to a position 4.0 cm distal to the SFJ. The cyanoacrylate is injected endovenously whilst compression is applied by the ultrasound probe. Two injections of 0.09 mL are given 1 cm apart, followed by a 3 minute period of local compression. This is then repeated with injections at 3 cm intervals and a 30 second ultrasound probe compression time until the intended length of the vein is treated. After completion, duplex ultrasound is performed to confirm occlusion of the GSV, and patency of the femoral vein. Small stab avulsions of varicosities are performed under local anaesthesia to complete the treatment.
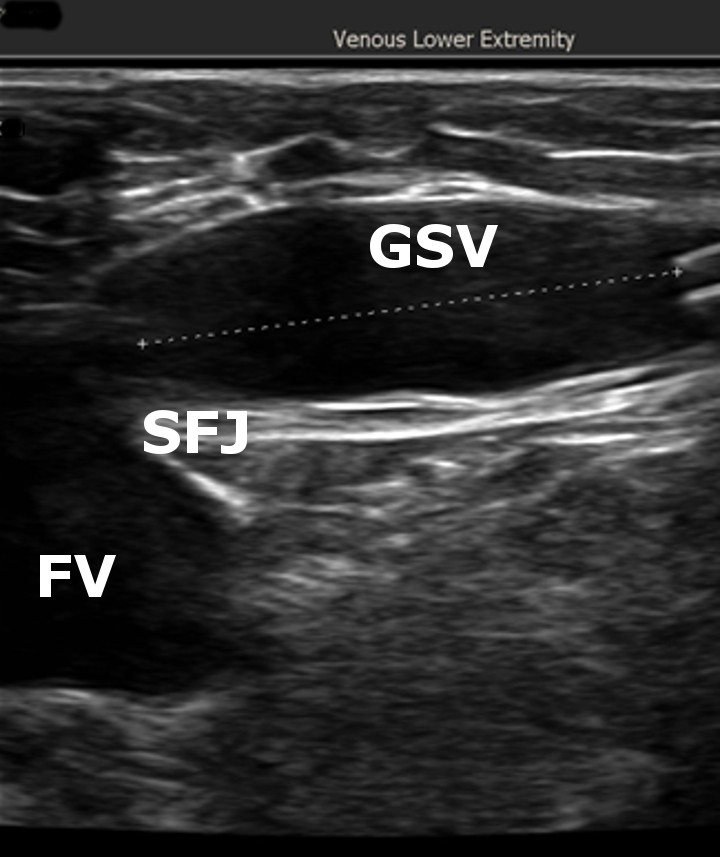
The catheter tip is seen 4 cm distal to the sapheno-femoral junction (SFJ) in preparation for glue deployment. GSV, great saphenous vein; FV, femoral vein.

The glue is deployed under ultrasound guidance whilst the assistant compresses the vein with the ultrasound probe