



This is an abbreviation for Ambulatory Venous Pressure and its measurement is considered the gold standard investigation in the assessment of chronic venous insufficiency (CVI). This relies on the hypothesis that increased venous pressures over time causes the discomfort and skin changes associated with CVI. The pressure is caused by the failure of the anti-gravitational mechanisms of the leg. This results in a hydrostatic column of blood exerting the highest pressure at the lowest point. Measurement of AVP is invasive and is taken from the dorsal foot vein or less commonly from the saphenous vein. AVP has been shown to mirror calf pump pressure changes.
SESHADRI RAJU The resting pressure in the dorsal foot vein approximates 90 mm Hg, representing the pressure of the blood column extending to the heart level. As the patient raises the heel to stand on the toes (tip-toe) rhythmically ten times, the resulting venous pressure curve is recorded (image below). Points of interest include the resting pressure (A), initial pressure spike (B), pressure nadir or ambulatory venous pressure (C), and time in seconds when pressure recovery had reached 90% of the resting level (VFT90). A pressure drop (% drop) of < 50% and a VFT90 <20 seconds are considered abnormal.
Venous reflux, which results in premature refilling and shortens VFT90 is a common cause of calf pump decompensation. Other calf pump abnormalities include increase or decrease of resting venous volume, ejected volume and calf pump compliance. Not only ambulatory venous pressure, but volume measurements with air-plethysmography are necessary to properly analyse calf pump abnormalities.
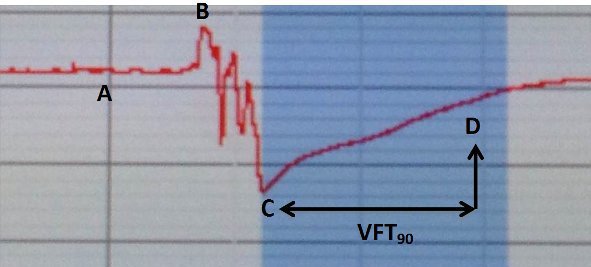
A – Resting Pressure
B – Initial Pressure Spike
C – Ambulatory Venous Pressure
D – VFT