



It is often stated that ultrasound competence of the terminal valve (TV) with incompetence of the pre-terminal valve (PTV) indicates that the source of great saphenous vein (GSV) reflux is from pelvic veins. In consequence, ligation of the sapheno-femoral junction alone will not prevent reflux of pelvic origin from entering the lower segments of the GSV.
It is important to determine whether the reflux source is from pelvic origin because GSV ablation or surgical stripping also may not be adequate in preventing pelvic venous reflux from entering the leg. The treatment of CVI from PVR should be achieved at a higher level. For example, pelvic vein embolisation, perineal foam sclerotherapy or perineal/inguinal escape point ligation. A careful assessment of the sapheno-femoral junction is required to discriminate competence between the TV and PTV and to make a confident diagnosis that the TV is fully competent. Elevation/dependency and Valsalva manoeuvres may compliment calf compression/release manoeuvres in the assessment of these valves.
DOMINIC MÜHLBERGER Terminal and pre-terminal valves are the most important valves of the GSV. Terminal valves are located at the sapheno-femoral junction. They should prevent reflux of blood from the common femoral vein (CFV) into the GSV. Pre-terminal valves are located between 1.5 and 8 cm distal to the sapheno-femoral junction. They should prevent reflux of blood arising from the confluence of the superficial inguinal, pudendal and accessory saphenous veins into the lower segments of the GSV. Both valves exist in about 90% of legs. However, the presence of these valves does not imply that all are fully competent.
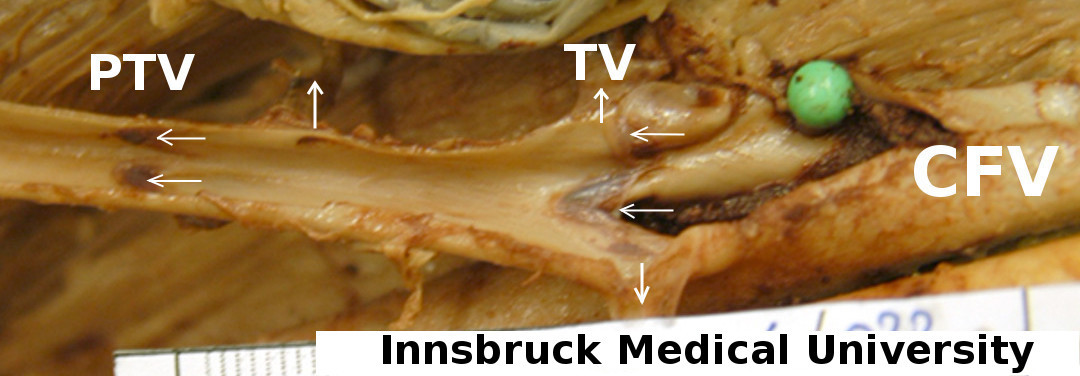
Cadaver dissection exposing the pre-terminal valve (PTV) and the terminal valve (TV) leaflets (horizontal arrows). Several tributaries are seen draining into the intervening segment (vertical arrows). With kind permission, Division of Clinical and Functional anatomy, Department of Anatomy, Histology and Embryology, Innsbruck Medical University.