



This is the endovenous closure of the saphenofemoral junction (SFJ) using a laser fibre. It is the endovenous equivalent of a traditional surgical crossectomy where the great saphenous vein (GSV) termination was ligated flush with the femoral vein using an incision in the groin.
IMRE BIHARI This has been performed by me and by some Eastern European colleagues for 10 years on about 5000 legs. It has proved to be safe and effective.
Over the last century many studies have been published about the necessity of crossectomy in the treatment of varicose veins. This was performed to interrupt all reflux sources down into the leg. However, after standard laser surgery many recurrences arise also from the SFJ. This prompts the need for an endovenous crossectomy technique in order to reduce groin recurrences.
The aim is to occlude the termination of the saphenous vein flush with the femoral vein. If this is not technically possible, and a short stump remains, this is still above the ascending tributaries which have the potential to provide descending reflux pathways down the leg.
Laser crossectomy has proved to be effective in the prevention of early recurrence and has reduced the ratio of recurrent groin reflux versus other sites of recurrence. The risk of an endothermal heat induced thrombosis (EHIT) is reduced using the appropriate tumescence method and with temporary anticoagulation. After several months, an apparent flush occlusion can lead to a stump of only a few millimetres. This is a benign finding resulting from clot retraction.
The aim is to close the saphenous vein flush with the femoral vein. As the laser fibre is withdrawn the tributaries are closed as well. Complete occlusion or a short stump effectively decreases junctional recurrence, especially in the early years. This is because junctional veins, like the anterior accessory saphenous vein or other ascending tributaries, are no longer available as a potential downward reflux pathway. In contrast to open surgical crossectomy, endothelial cells are not released from divided veins or injured lymph nodes. This reduces the incidence of a neovascularisation as a further source of recurrence.
Our technique for laser crossectomy is as follows:
- The tip of the laser fibre should be 0.5 cm from the femoral vein. A ring fibre is recommended for precise placement. This is in contrast to the 2 cm distance advocated for a standard procedure.
- Over twice as much laser energy delivery is recommended for the first 3 cm next to the junction (about 200 J/cm). This is because of the higher venous pressure and larger GSV calibre at its termination. Higher energy is recommended to cause serious damage to the vein wall, but some of this is off-set by the large amount of cold tumescence necessary which decreases the effectiveness of the thermal injury. The rest of the refluxing GSV is then ablated using a lower energy delivery tailored to the calibre and thickness of the vein.
- A higher amount (10 ml/cm) of cooled tumescent solution (4 °C) is recommended to compress the SFJ region. This is to decrease the amount and temperature of the steam and hot blood flowing into the femoral vein.
- Subcutaneous low molecular weight heparin (LMWH) for 5 days.
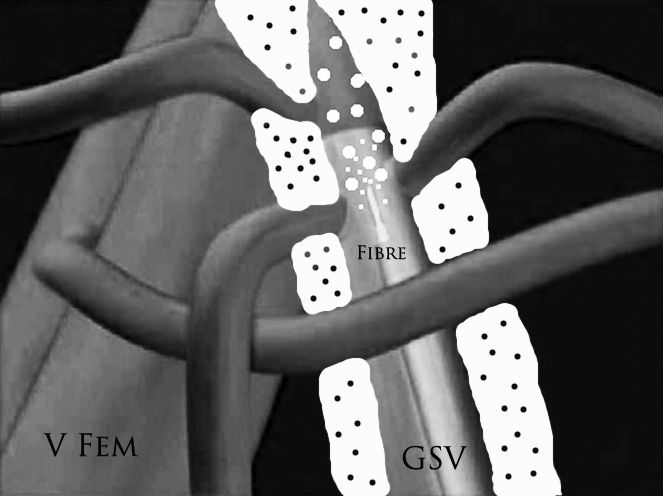
Fig 1. Tumescent solution (black dots on white) is shown compressing the junctional part of the GSV prior to its entry in to the femoral vein (V FEM).
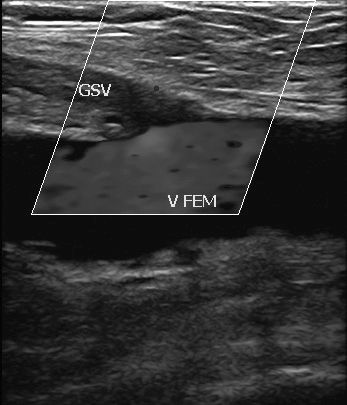
Fig 2. Occlusion of the GSV flush with the femoral vein (V FEM).