



Pelvic congestion syndrome is a collection of symptoms and signs which occur when the pelvic veins fail in their drainage function. The cause is usually through reflux but venous obstruction may be responsible in some cases. The increase in pelvic venous volume and pressure can be transmitted into the legs through pelvic escape points resulting in venous leg symptoms and varicose veins.
PIER-LUIGI ANTIGNANI Pelvic congestion syndrome (PCS) is a chronic venous disease that affects the ovarian, internal iliac and perineal plexuses. It is responsible for up to 40% of chronic pelvic pain cases and represents a condition affecting almost 10% of the population.
The symptomatology can become extremely debilitating because of the chronic lower abdomen pain, dyspareunia, abdominal and/or pelvic tenderness, dysmenorrhea, lumbosacral neuropathy, urinary frequency and rectal discomfort. Occasionally the mucosal congestion may result in haemorrhoids and haematuria. Patients usually present first to a gynaecologist. After extensive gynaecological investigations a venous specialist may be consulted when the diagnosis becomes established.
A detailed clinical history is fundamental to address the correct clinical suspicion. However, the symptoms may be non-specific with some overlap between true gynaecological symptoms and those of PCS.
A pelvic echo colour Doppler is mandatory to provide a clear diagnosis of PCS according to well defined parameters. This includes a trans-abdominal ultrasound as well as a trans-vaginal ultrasound in various positions using different provocation manoeuvres. Magnetic resonance imaging (MRI) is often involved in the diagnostic process. It is non-invasive, can identify engorged veins and is valuable in ruling out other pathologies involved with PCS. A diagnostic venography is useful not only for the definition of the disease, but also for its potential therapeutic solution by percutaneous pelvic veins embolisation with coils and sclerosant foam.
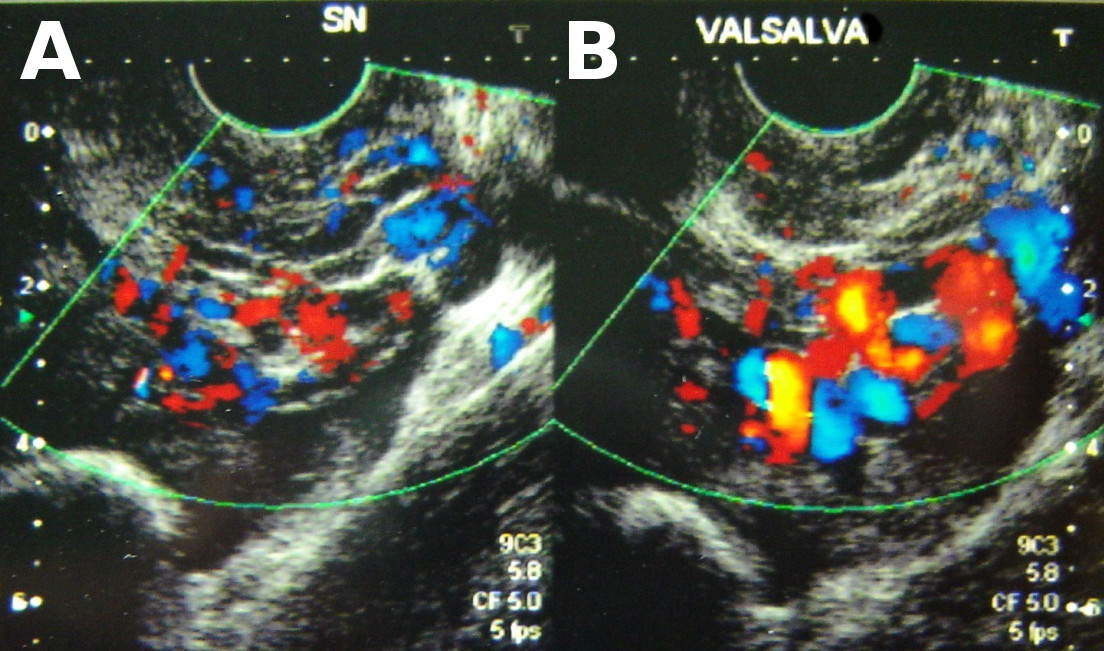
Trans-vaginal ultrasound in the reclining position at rest (A) and during a Valsalva manoeuvre (B). Note the engorged veins in B which appear to occupy a large amount of the left pelvic volume.
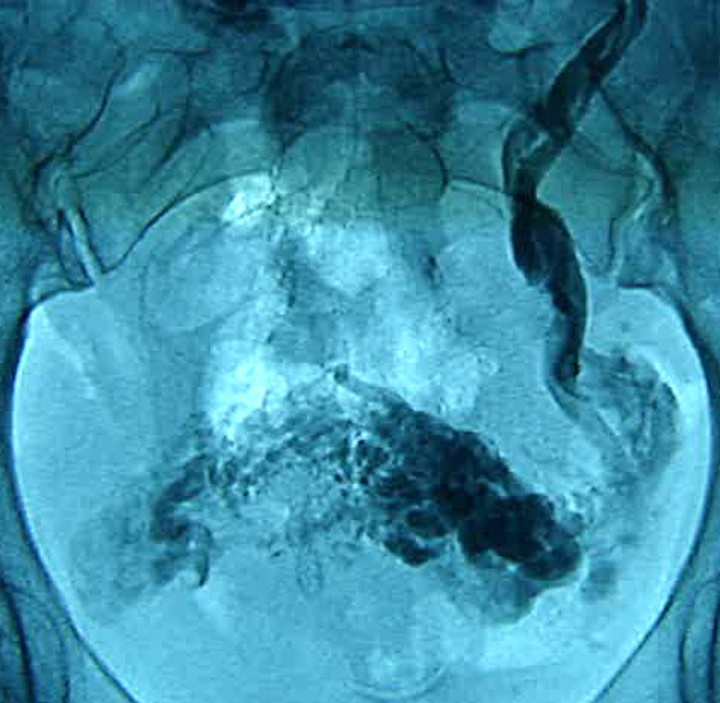
Selective left ovarian vein venogram in the same patient. Large calibre ovarian veins are shown with retrograde flow down into the pelvis. Note cross-filling of the contralateral pelvic veins.