



Pelvic venous reflux (PVR) may cause prolonged pressurisation of the veins in the pelvis. This can result in pelvic congestion syndrome (PCS) with non-cyclical pain or a constant dull ache, exacerbated standing or sitting, for over 6 months. It may be associated with dyspareunia and haemorrhoids. If the reflux escapes into the leg it may lead to varicose veins or chronic venous disease (CVD). Like the perforating veins in the thigh and calf, these leak points may be a target for ultrasound guided foam sclerotherapy (UGFS). Perineal or P-point sclerotherapy aims to ablate the source of this reflux arising down from the pelvis.
FRANCESCO ZINI The perineal escape of reflux arises from the internal pudendal vein(s) which pierces the superficial perineal fascia (Colles’ fascia) at the level of the superficial transverse perineal muscle. The anatomical term for this channel is the pudendal canal (Alcock’s canal). Clinically, this is recognized by varicose veins near the junction between the labia majora and thigh, just anterior to the buttock skin crease.
Lorenzo Tessari and myself have extensive experience of P-point sclerotherapy. It is an alternative to the surgical approach practiced by Claude Franceschi and Amine Bahnini. The P-point is located using colour duplex ultrasound whilst the patient is in the lithotomy position. Reflux is confirmed using a Valsalva manoeuvre. The distance from the skin to the P-point is measured to establish the depth of the needle required for injection. Fresh foam is prepared using the Tessari method by agitating 2% sodium tetra-decyl sulphate (STS) in CO2 (70%) and O2 (30%). The volume required is a judgment which depends on the size and extent of the veins, and the feedback from the probe of the foam filling the veins. A 88% obliteration rate is reported after 5 years, with 23% requiring a second stage injection at 3 weeks.
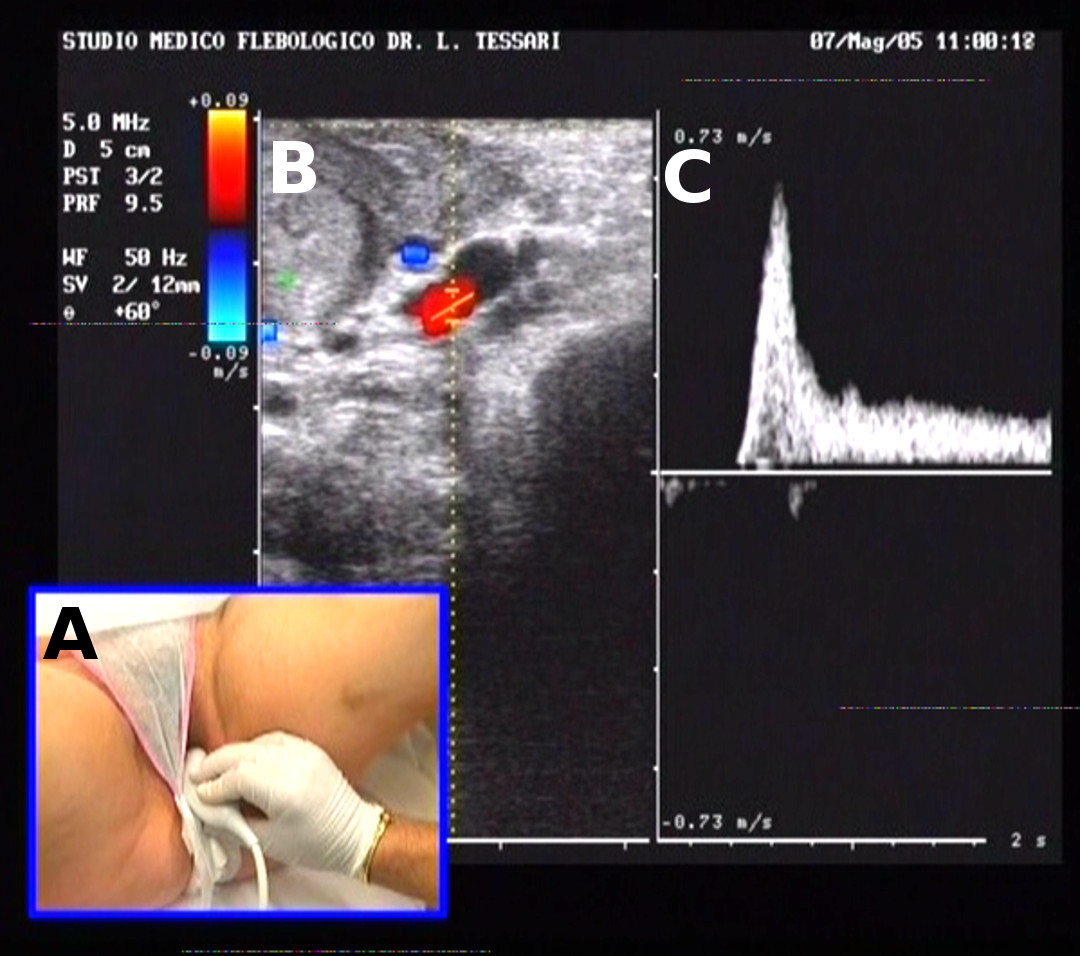
Diagnosis: A) the ultrasound probe is positioned transverse between the ischio-pubic bone and the posterior vagina. B) Reflux is visualised as red. C) The reflux is prolonged.

Treatment: A) echo guided puncture of the P-point. B) injection of fresh foam with acoustic shadows (arrows).