



Factor V is part of the normal coagulation cascade which promotes the production of a fibrin thrombus. Its action is inactivated by activated protein C (APC), thereby preventing thrombosis. This is the normal situation in health. Factor V Leiden (FVL) is a mutation. It is an autosomal dominant condition with incomplete penetrance. Patients with an abundance of FVL retain the pro-coagulation properties of Factor V but, because of a defect in the receptor, are unable to bind the inactivator APC. This results in a hyper-coagulation state with a tendency towards thrombosis. The FVL, whilst causing a hyper-coagulation state, does not seem to be associated with a great increase in pulmonary embolism (PE). This paradox is described below.
JANA HIRMEROVA Venous thrombo-embolism (VTE) may manifest as isolated deep vein thrombosis (DVT), isolated pulmonary embolism (PE), or both DVT and PE. Factor V Leiden (FVL) is the most common hereditary cause of thrombophilia in Caucasians. This disease seems to be associated with more frequent presentations of DVT and less frequent presentations of symptomatic PE. This is a paradox because hyper-coagulation states would be expected to have a proportionate increase in the incidence of PE. Several possible mechanisms of this phenomenon, named the FVL paradox, have been proposed.
FVL carriers may develop thrombi of smaller size which are more often located distally and therefore less prone to embolise. However, some authors have reported a higher prevalence of proximal DVT in FVL patients, thereby lessening the credibility of a smaller thrombus hypothesis.Other hypothesis assumed a higher frequency of fatal PE in FVL carriers and consequently a lower prevalence of FVL in PE survivors. However, autopsy studies have not supported this explanation. Furthermore, heterozygosity for FVL is compatible with extreme old age. Finally, thrombus in FVL carriers is supposedly more stable and more adherent to a vessel wall, perhaps due to enhanced local thrombin generation.
In summary, the observation of the FVL paradox appears to be real, however the exact patho-physiological explanation of this phenomenon requires further research.
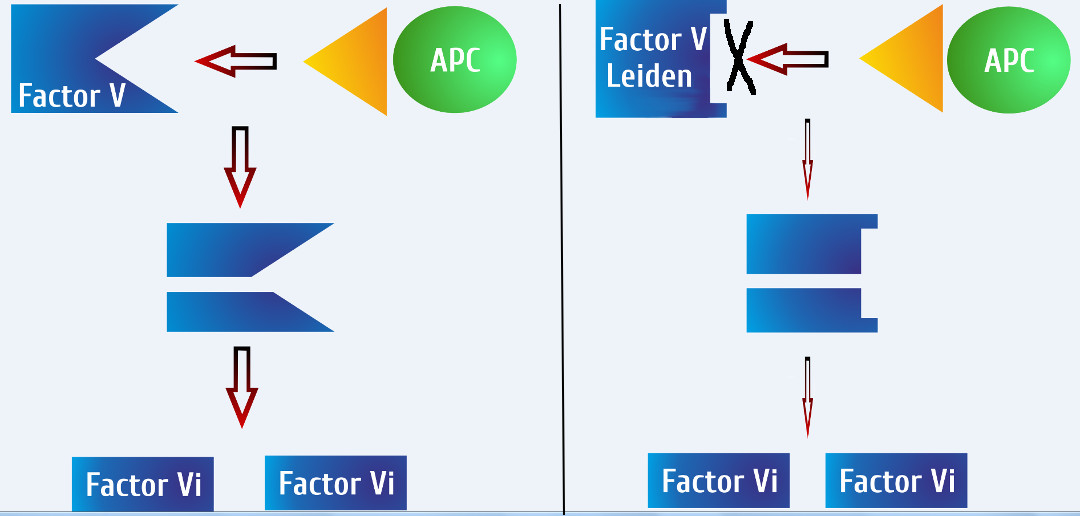
A small change in the Factor V molecule into the FVL mutation hinders the binding of activated protein C (APC). Consequently, the cleavage of FV into two inactive fragments (Factor Vi) by APC is substantially diminished.