



Popliteal vein compression (PVC) is rarely considered as a cause of venous obstruction, chronic venous insufficiency or even DVT. Greater awareness of the condition may lead to an improved diagnosis in patients with venous disease.
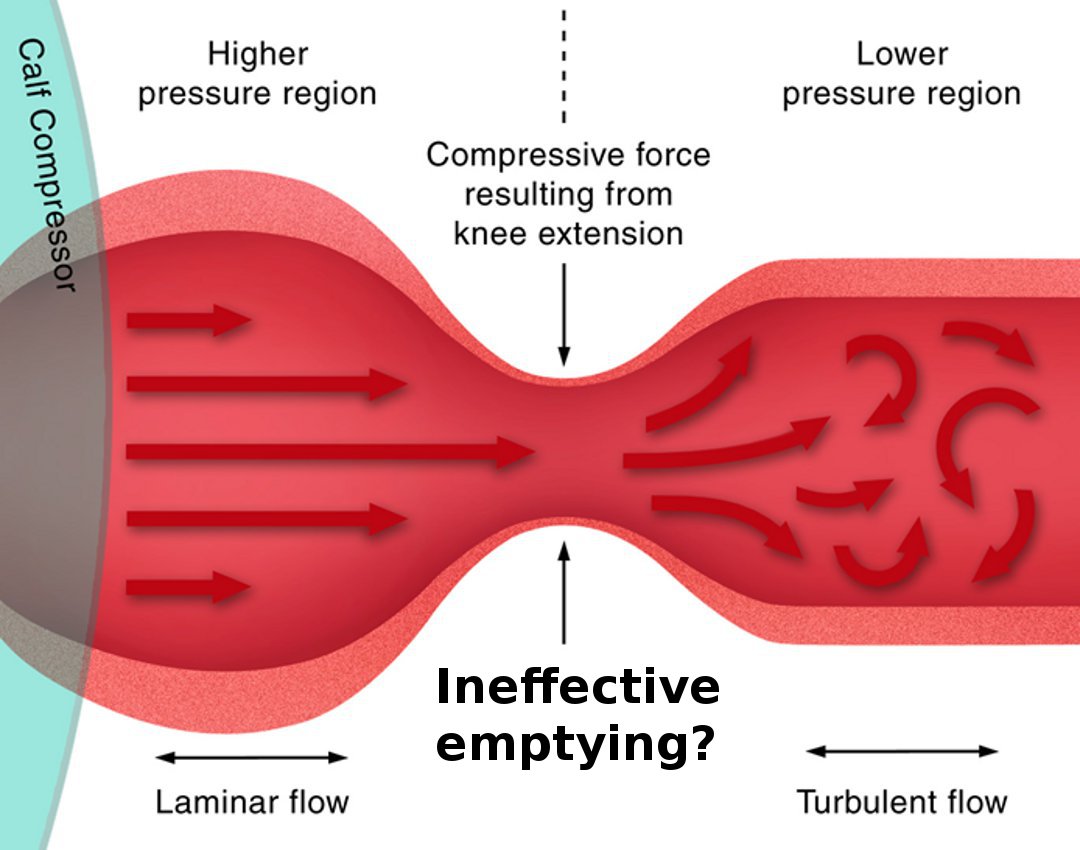
DAVID HUBER This condition is distinct from popliteal vein entrapment. Popliteal vein compression is seen when the knee is extended or locked. It is caused by high pressure within the popliteal fossa as one of the bellies of gastrocnemius encroaches on the popliteal fossa resulting in compression of the popliteal vein (which is a low pressure structure). It occurs in around 17% of subjects and is particularly prevalent in surgical patients who are supine and under anaesthetic, where the incidence is around 64%. It is likely that this contributes to an increase in the likelihood of perioperative DVTs. Recent publications suggest that it is associated with lipodermatosclerosis, chronic venous stasis, and increasing the likelihood of developing a DVT. It is interesting to note that at the end of a stride, the knee is fully extended (causing PVC in some subjects) at the time that the calf contracts. This may cause reversed flow in perforators and contribute to retrograde incompetence in the great saphenous vein and the development of varicose veins. Clearly further research is required to more completely understand the pathophysiology of PVC.
 Popliteal vein compression
Popliteal vein compression