



This is an abbreviation for Endo-Venous Laser Ablation. It is a widely practiced technique for treating varicose veins. It is usually performed using a local anaesthetic whilst the patient lies on an operating table. A laser fiber is inserted along the length of the saphenous vein, which is usually the main vein from which varicose veins arise. Before firing the laser fiber, the patient is positioned head down and legs up to empty the veins of blood. The heat from the end of the laser fiber tip destroys the vein as it is pulled out slowly. Associated varicose veins frequently need treatment at the same session, either by pulling them out through small cuts in the skin or by injecting them with foam. Occasionally they disappear on their own after EVLA. A pre-operative test which can identify those patients requiring concomitant phebectomies and those patients whose veins disappear spontaneously after EVLA would be an interesting topic to investigate as a future research project.
VICTOR CANATA We have been performing laser treatments for varicose veins in Paraguay for more than ten years on over 1500 patients, with an excellent record of saphenous occlusion (> 98% in 2 years) and safety. All treatments are performed in an office setting, using a 1470 nm wavelength laser fiber, 400 µm in diameter. The procedure is safe, easy to perform and well tolerated by the patient. No general or regional anaesthesia is required. Local anaesthetic is injected under ultrasound control to surround the vein with fluid (tumescence). This acts as a heat sink to protect surrounding tissues, nerves and skin from thermal injury. The procedure has higher rates of acceptance than conventional surgical stripping with a faster return to normal activities. Groin access is not required so there are no wounds to heal at this location. Our achievement in excellence in technique and cost-effectiveness include the use of a large, high resolution monitor for detailed visualisation, and our commitment to a standardised efficient working environment.
The laser delivers energy to destroy the refluxing great saphenous vein (GSV) at a power setting of 9 – 14 Watts. The fiber is positioned 1 cm below the sapheno-femoral junction (SFJ) and fired in pulses, with a pull-back speed depending on the diameter of the vein to be destroyed. We aim for an energy delivery of about 70-90 Joules/cm. The vein is checked with ultrasound during and after completion to confirm a successful ablation. Patients are instructed to resume daily activity and to wear stockings for one week. In the unlikely event of a saphenous recanalisation at the one week follow-up, we can repeat the procedure using a higher energy delivery rate.
Continued evaluation and long term follow up are required to define the complete role of the laser in the treatment of varicose veins.

EVLA in an office based environment.

Transillumination provides feedback on the location of the tip of the laser fiber which is seen here in the mid-thigh part of the great saphenous vein.
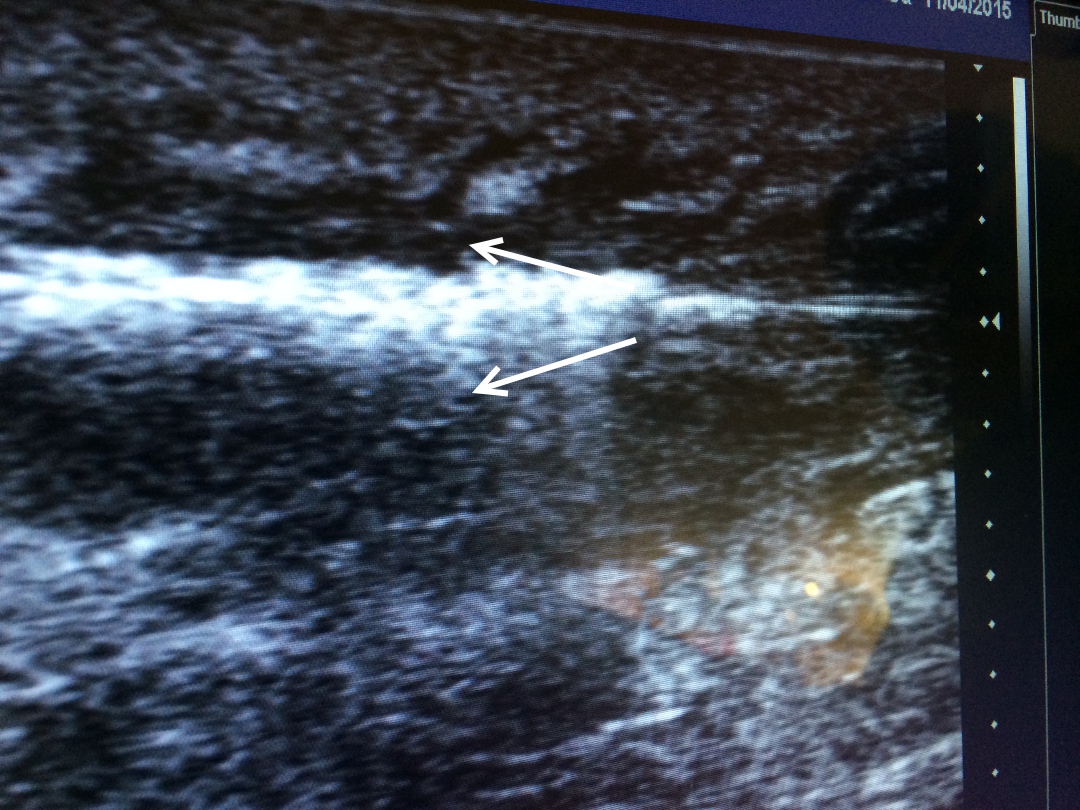
Bubbles of gas released from a laser fibre during its action in ablating a GSV. The laser fibre tip is seen at the base of the arrows and is being withdrawn from left to right.